Table of Contents
What is SHAPU Eye Disease?
Seasonal hyperacute panuveitis (SHAPU) is a mysterious eye disease seen and reported only in Nepal since 1975. An important cause of unilateral childhood blindness. It is the most devastating intraocular inflammatory disease which leads to loss of sight within a week and, in many cases disfigurement later.
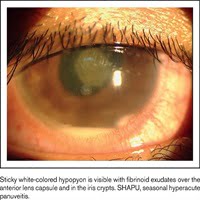
Within a few days, the eye becomes soft with shallowing of anterior chamber which has been called “Malignant Hypotension”. Hypopyon, fibrinous exudates in the anterior chamber, a difficult to dilate pupil and inability to visualize retina because of massive exudation into vitreous producing a “White pupillary reflex in Red eye” with little or no pain are other characteristic features of the disease.
Etiology
Most data on etiology rely solely on contact history with a suspected agent (moths) and there is evidence suggesting that the disease is due to exposure to possible toxins. But with more cases – not all agree to the existing knowledge.
While etiopathogenesis is still debated, the data from researchers do agree on some key peculiarities. SHAPU usually affects one eye, has a cyclic epidemic pattern occurring during the period of the end of the monsoon (August-September) and the beginning of severe winter (December-January).
The disease still remains a mystery with no hard evidence of its source. So far, the management protocol or treatment has been limited. SHAPU continues to delude – and continues be to most devastating inflammatory eye disease rendering eye functionless within a week.
Primary prevention
Currently, the only primary prevention is to avoid contact with moths during the seasons of epidemicity.

Clinical Features of SHAPU
Most of the clinical symptoms and signs of SHAPU are non-specific.
Symptoms of SHAPU Eye disease
- Sudden onset of redness with minimal pain*
- White pupillary reflex (leukocoria) in a red-eye *
- Unilateral involvement
- Decreased vision
Signs of SHAPU eye disease:
- Circumciliary congestion
- Leukocoria
- Fibrinoid anterior chamber reaction
- Hypopyon
- Shallow Anterior chamber
- Collection of fibrinoid exudates in the crypts of muddy iris
- Decreased intraocular pressure (malignant hypotension)*
- Retinal assessment is difficult
Footnote – * Hallmark in most cases
The major clinical finding of SHAPU
- White pupillary reflex in Red eye
- Little or no pain
- Almost always unilateral
- Rapid and profound loss of vision.
others clinical features
- Malignant Hypotension
- Children predominantly
- Hypopyon, fibrinous exudates in anterior chamber.
- A difficult to dilate pupil and inability to visualize retina
Laboratory test
Specimen collection
- Specimens-vitreous fluid, aqueous fluid, conjunctival swab, blood
- Specimens should be collected by ophthalmologists in the operation theatre maintaining the sterility.
- Both diluted and undiluted vitreous fluid should be collected in a sterile syringe.
- The conjunctival swab should also be collected from both eyes. It serves as control when comparing with the ocular fluid samples
- The blood sample is collected to rule out endogenous endophthalmitis
Differential diagnosis
The differential diagnosis, therefore, may include a range of entities.
- Infectious conditions
- Endogenous endophthalmitis
- Exogenous endophthalmitis
- Herpetic retinitis
- Tuberculosis
- Syphilis
- Fungal infection in drug users
- HIV retinopathy
- Toxoplasmosis
Immunological conditions
- Sarcoidosis
- Multiple evanescent white dot syndrome (MEWDS)
- Behcet’s disease
Read more articles about SHAPU
For more details about SHAPU medical and surgical management: Click here to read more
New Clinical and Laboratory Findings of SHAPU
Disclaimers: This article is for educational purpose only and references were taken from various sites. Please comment below for any copyright issues or any recent updates on SHAPU.